



 Publications
Publications
 Partners
Partners


Cardiovascular disease (CVD) is the single largest cause of mortality worldwide, accounting for 18 million deaths per year globally.
Call for more affirmative action
In the past few years, notable progress has been made in treating CVD and a decline is evident due to early detection strategies, advanced medical treatment, and risk factor reduction.
However, the trend towards unhealthy lifestyles persists, hampering medical progress, and calling for more affirmative action to prevent such disease.
The main component of cardiovascular disease is Coronary Artery Disease (CAD).
Read: Exercise key to a healthy heart
CAD is a progressive, chronic disease which affects the inner lining of the coronary arteries. There is a build-up of atherosclerotic plaque which narrows the arteries and obstructs normal blood flow.
Atherosclerotic plaque can be either active and unstable, or quiet and stable. Unstable plaques, even mild- to moderate-sized plaques can tear, rupture, swell, or undergo a combination of these processes and can result in a sudden and complete obstruction of a coronary artery, leading to an acute myocardial infarction (heart attack).
Non-modifiable and modifiable risk factors for heart disease
Non-modifiable risk factors for CVD cannot be changed. These factors include:
- Age
- Gender
- Family history
People who are generally at a higher risk for CVD are male, above the age of 50 years, or have a family history of premature CVD (male before 55 years of age, female before 60 years).
Read: Put your heart into it
On the other hand, modifiable risk factors for CVD can be changed predominantly through healthy lifestyle modifications. The modifiable risk factors include:
- Obesity (BMI ≥30 or waist circumference >94 cm for men; >80 cm for women)
- Smoking
- Cholesterol levels
- Hypertension (140/90mmHg or higher)
- Diabetes
- Lack of exercise
- Unhealthful diet
Modifiable risk factors are shown to be increasingly prevalent in South Africa, contributing significantly to alarming cardiac risk factor profiles.
What can be done to reduce your risk?
Exercise and a healthy diet are considered the two most important components of lifestyle modifications that can significantly reduce your risk for CVD.
Following a structured routine of frequent exercise can hold many benefits including:
- Decreased blood pressure
- Decreased resting heart rate
- Lower cholesterol levels
- Decreased stress and anxiety
- Weight loss
- Improved heart and lung function
Exercise has been identified as a central element of cardiovascular disease risk reduction and lifestyle modification. It can bring about improved physical performance, reduced symptoms, and improved quality of life.
In secondary prevention, regular training constitutes an important factor that positively affects the prognosis of illness.
Exercise training has been shown to have direct benefits on the heart and coronary vasculature, including myocardial oxygen demand, endothelial function, autonomic tone, coagulation and clotting factors, inflammatory markers, and the development of coronary collateral vessels.
The mechanism for reduced cardiovascular mortality in patients who have received exercise-based cardiac rehabilitation is not clear, but may be due to improved myocardial revascularization, protection against fatal dysrhythmias, improved cardiovascular risk factor profile, improved cardiovascular fitness, or increased patient surveillance.
Recommended exercise programme
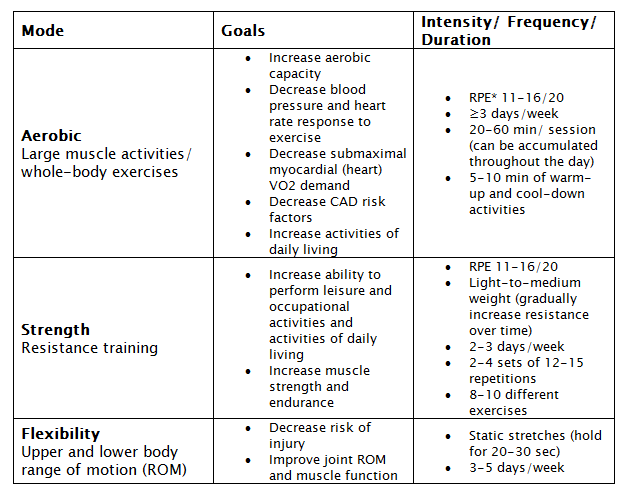
*RPE = rating of perceived exertion (how tiring/hard the exercise feels to you). Scale from 6-20. 7= very, very light; 9= very light; 11= fairly light; 13= somewhat hard; 15=hard; 17= very hard; 19= very, very hard.
If you do have any of the risk factors for heart disease, you should consult your doctor before embarking on any kind of exercise programme. You should also consider having a biokineticist help you to prepare a programme that is scientifically based and tailored to your condition and needs.
Read more:
References
1. Ortegon, M., Lim, S., Chisholm, D. & Mendis, S., 2012. Cost effectiveness of strategies to combat cardiovascular disease, diabetes, and tobacco use in sub-Saharan Africa and South East Asia: mathematical modelling study. BMJ, 344(607), pp. 1-15.
2. Ramli, A. et al., 2014. Study protocol of EMPOWER Participatory Action Research (EMPOWER-PAR): a pragmatic custer randomised controlled trial of multifaceted chronic disease management strategies to improve diabetes and hypertension outcomes in primary care. BMC family Practice, 15(151), pp. 1-16.
3. Owolabi, M. et al., 2014. Understanding the rise in cardiovascular diseases in Africa: harmonising H3Africa genomic epidemiological teams and tools. Cardiovascular Journal Of Africa, 25(3), pp. 134-136.
4. Noubiap, J., Jingi, A. & Kengne, A., 2014. Local innovation for improving primary care cardiology in resource-limited African settings: an insight on the Cardio Pad project in Cameroon. Cardiovascular Diagnosis and Therapy, 4(5), pp. 397-400.
5. Sliwa, K. et al., 2008. Spectrum of heart disease and risk factors in a black urban population in South Africa (the Heart of Soweto Study): a cohort study. Lancet, 371(9616), pp. 915-922.
6. Heran, B. et al., 2014. Exercise-based cardiac rehabilitation for coronoary heart disease. Cochrane Database Systermatic review, 7(CD001800), pp. 1-73.
7. Muller-Riemenschneider, F. et al., 2009. Evaluation of medical and health economic effectiveness of non-pharmacological secondary prevention of coronary heart disease. GMS Health technology Assessment, 5(10.3205), pp. 1-12.
8. Yusuf, S. et al., 2014. Cardiovascular Risk and Events in 17 Low-Middle-, and High-Income Countries. The New England Journal of Medicine, 371(9), pp. 818-827.
9. Hanson, M. et al., 2013. Coronary Artery Disease. Primary Care Clinical Office Practitioners, 40(8), pp. 1-16.
10. Mensah, G., 2008. Ischaemic heart disease in Africa. Heart, 94(7), pp. 836-843.
11. Tibazarwa, K. et al., 2009. A time bomb of cardiovascular risk factors in South Africa: Results from the Heart of Soweto Study "Heart Awareness Days". International Journal of Cardiology, 132(2), pp. 233-239.
12. Damasceno, A. et al., 2012. The Causes, Treatment, and Outcome of Acute Heart Failure in 1006 Africans From 9 Countries. Arch International Medicine, 172(18), pp. 1386-1394.
13. Mayosi, B. et al., 2009. The burden of non-communicable diseases in South Africa. Lancet, 374(9693), pp. 934-47.
14. Stewart, S. et al., 2006. Mapping the emergence of heart disease in a black, urban population in Afrcia: The Heart of Soweto Study. International Journal of Cardiology , 108(1), pp. 101-108.
15. Mayosi, B. et al., 2009. The burden of non-communicable diseases in South Africa. Lancet, 374(9693), pp. 934-47.
16. Stewart, S. et al., 2006. Mapping the emergence of heart disease in a black, urban population in Afrcia: The Heart of Soweto Study. International Journal of Cardiology , 108(1), pp. 101-108.
17. Moran AE, 2014. Variations in ischemic heart disease burden by age, country, and income: the Global Burden of Disease, Injuries, and Risk Factors 2010 study. Global Heart, 9(1), pp. 91-99.
18. Tollman, S. et al., 2008. Implications of mortality transition for primary health care in rural South Africa: a population-based surveillance study. Lancet, 372(9642), pp. 893-901.
19. Dalal, S. et al., 2011. Non-communicable diseases in sub-Saharan Africa: what we know now. International Journal of Epidemiology, 40(4), pp. 885-901.
20. Popelova, J., Brtko, M. & Nemec, P., 2013. Summary of the ESC guidelines on the management of valvular heart disease (version 2012). Prepared by the Czech Society of Cardiology.. Cor et Vasa, 55(16), pp. 141-156.
21. Sforzo, G., Moore, M. & Scholtz, M., 2015. Delivering Change that Lasts. ACSM's Health and Fitness Journal, 19(2), pp. 20-27.
22. Gagliano, M., 1988. A Literature Review on the Efficacy of Video In Patient Education. Journal of medical Education, 63(10), pp. 785-792.
23. Banda, D., Libin, A., Wang, H. & Swain, S., 2012. A Pilot study of a culturally targeted video intervention to increase participation of African American patients in cancer clinical trials. The Oncologist, 17(3), pp. 708-714.











